The AH&MRC calls on the NSW Government to address the mental health and social and emotional wellbeing needs of Aboriginal people across NSW in the upcoming budget.
In 2019 – 2020, Aboriginal people in NSW have endured displacement and destruction of their communities due to bushfires, floods, drought, and COVID-19. Aboriginal people experience these traumatic events in addition to the transgenerational trauma that exists from colonisation, loss of land and language and cultural practices.
The Aboriginal Health & Medical Research Council (AH&MRC) and its Member Services work to address the Social and Emotional Wellbeing (SEWB) and mental health needs of Aboriginal people across New South Wales. Unfortunately, not all Aboriginal Community Controlled Health Organisations (ACCHOs) in NSW have sufficient funding to ensure communities are kept safe and maintain resilience to manage the past, current, and emerging environmental challenges, and disparities.
In April 2020, The NSW Government committed an additional $73 million to mental health support packages which included: 180 additional specialist, community-based mental health clinicians, expansion of the virtual mental health program to all Local Health Districts, free access to Tresillian’s digital SleepWellBaby program, 60,000 extra calls to the 1800 NSW Mental Health Line and pop-up mental health Safe Space sites. The AH&MRC, on behalf of the NSW ACCHO Sector, is calling for an increase in funding to provide and develop culturally appropriate SEWB and Mental Health services and programs.
Under the Close the Gap Agreement 2020, the NSW Government has committed to addressing the SEWB and mental health needs of Aboriginal people. This is a priority area to be addressed in the initial five policy partnerships.
“Aboriginal people access culturally appropriate services through our Aboriginal Community Controlled Health Organisations (ACCHOs). It is vital for our ACCHOs as a key health service providers in NSW to be adequately resourced to provide these essential services, which is part of a holistic care model that is unique to our sector,” said Robert Skeen, CEO AH&MRC.
About us
The AH&MRC assists ACCHOs across NSW to ensure they have access to an adequately resourced and skilled workforce to provide high-quality health care services for Aboriginal communities. As the Peak Body for Aboriginal Health in NSW the AH&MRC represents the rights and interests of 47 Member Services.
For more information or media enquiries, please contact:
Nadia Ruben
Communication and Marketing Manager AH&MRC
E: nruben@ahmrc.org.au | T +61 2 9212 4777
AH&MRC’s NAIDOC Week Portrait Series celebrates the skills, strength and diversity of Aboriginal people working in the Aboriginal community-controlledhealthcare sector
The Aboriginal Health and Medical Research Council (AH&MRC) NADIOC Portrait Seriesprofiles five Aboriginal people who have each made a significant contribution to the health and wellbeing of Aboriginal people in NSW. The five nominees were selected based on nominations received from Community members, and people working in the sector.
Aboriginal photographer and proud descendant of the Wiradjuri and Yuwaalaraay Nations, Marley Morgan travelled across NSW to capture the portraits of Phillip Naden, Uncle Terrence Donovan, Steven Taylor, Donna Taylor, and Melanie Briggs in their local Community.
Each nominee, in their own words,shared what this year’s theme, ‘Always Was, Always Will Be’meansto them. Their words capture their individual journeys and what it means to be part of the world’s oldest, continuous culture.
Phillip Naden, Coonamble Aboriginal Medical Service
“Always was,always will be were not words I heard as a young person, but as time goes on and my living status, memory and tradition changes, so have our conversations.” said Phillip Naden.
Melanie Briggs, Waminda Aboriginal Medical Service
“The truth is we were always here, wandering this land for thousands of years. Even though science has proven it, we can feel it. It’s a power beyond this world that can only be felt by our people,” said Melanie Briggs.
Uncle Terrence Donovan, Elder and Member of the Aboriginal Health and Ageing Program at NeuRA.
“As a proud Gumbayngirr and Biripi man I am spiritually and culturally connected to this country. My ancestors have cared for it, from the time of creation and I have lived my culture every day,” said Terrence Donovan.
Donna Taylor, Pius X Aboriginal Corporation Clinic
“Always Was. Always Will Be means that our people were the first to walk on this continent and maintain connections to our culture and spirituality to this day, whether those connections are to the land or sea. We have been here from when time began and will be here well into the future,” said Donna Taylor
Steven Taylor, Weigelli Residential Rehabilitation Centre
Our connection to Country, water and sky have never been lost. Thanks to our Elders, the fire keeps burning within us all,” said Steven Taylor.
“I am so proud of the amazing work of Aboriginal people working in the sector. We are the healers of our Communities, working to improve the health and wellbeing of our people. Our shared goal of providing the best, culturally appropriate care to our people strengthens and unifies our sector.Robert Skeen, AH&MRC CEO.
To view the NAIDOC Week portraits and stories click here.
The AH&MRC) is the peak body for Aboriginal Community Controlled Health Organisations (ACCHO’s) across NSW.The AH&MRC is committed to ensuring that our 47 Member Services have access to the resources, funding and workforce to service the health needs of their Communities. We work alongside our ACCHO’s to ensure Aboriginal people in NSW have access to the best level of holistic healthcare.
In the past few weeks we have seen the inquest into the death in custody of Nathan Reynolds who died following an asthma attack, the conviction of a police officer for the assault of an 18 year old Aboriginal boy in police custody, and the referral of Dwayne Johnstone’s death to the Director of Public Prosecutions for investigation.
At the same time the NSW Parliament has commenced hearings for a new inquiry into oversight of deaths in custody and the mass incarceration of Aboriginal people. NSW CAPO calls on the Government to use this inquiry process as an opportunity to act without delay to rapidly and radically transform the justice system – Aboriginal peoples’ lives depend on it.
NSW CAPO calls on the NSW Government to end deaths in custody and the over-incarceration of our people. Urgent priorities for action include the immediate establishment of a Walama Court; independent investigations of all deaths in custody and police misconduct; raising the age of legal responsibility to at least 14; and the creation of ambitious state-based justice targets.
Almost 30 years ago, the Royal Commission into Aboriginal Deaths in Custody (RCIADIC) highlighted the mass incarceration of Aboriginal and Torres Strait Islander people across Australia. Since the RCIADIC, there have been numerous other Royal Commissions, inquiries, reports and recommendations which have focused on ending the imprisonment of Aboriginal and Torres Strait Islander people and preventing Aboriginal deaths in custody. Yet these reports continue to sit on the shelf gathering dust, and many of the recommendations remain unimplemented both in NSW, and other states and territories.
Deputy Chair of the NSW Aboriginal Land Council (NSWALC) and Co-Chair of NSW CAPO, Charles Lynch:
“Governments must shift from delivering systems predicated on disadvantage, to facilitating the aspirations, priorities and self-determination of Aboriginal peoples. This includes partnering with NSW CAPO to deliver whole-of-government reforms to the justice system.”
NSW AECG President and Co-Chair of NSW CAPO, Cindy Berwick:
“We know that connection to culture, community and education are key protective factors for our kids. We urgently need to end the school-to-prison pipeline, by raising the age of legal responsibility to at least 14 and investing in the supports our kids need to thrive”.
Deputy CEO of First Peoples Disability Network, June Reimer:“It is critical that dedicated resources are provided to Aboriginal community-controlled organisations to provide specialised and culturally appropriate support to Aboriginal people – including the co-location of disability support workers within Aboriginal legal services, to ensure the early detection and diversion of our people with disability away from the criminal legal system.”
CEO of the Aboriginal Health and Medical Council, Robert Skeen:
“Drug addiction should be treated as a health issue rather than a criminal justice issue. Without appropriate and timely rehabilitation and adequate diversionary programs, Aboriginal people proactively seeking treatment are forced into the criminal legal system.”
A/Executive Lead of AbSec – NSW Child, Family and Community Peak Aboriginal Corporation, Bill Prichard:
“It is important to look at the broader systemic issues that are forcing Aboriginal families and kids into the criminal justice system at vastly disproportionate rates. Aboriginal children in NSW are currently 11 times more likely to be removed from their families than non-Aboriginal children. Too often this results in them being forced into the quicksand of the youth justice system.”
”Sadly too often the road leads directly from Out of Home care to youth and adult incarceration.”
CEO of Link up NSW, Janelle Clarke:
“The legacy of past government policies of being separated from families and culture through forced removal, forced adoptions and being raised in institutions, has had long lasting impacts on our people and communities. Greater investment into supporting our people through culturally appropriate reunification programs, counselling services, and the use of circle sentencing such as Walama Court, would serve our people better than the harsh and unjust treatment they receive from the justice system.”
Chair of the Aboriginal Legal Service (NSW/ACT), Mark Davies:
“It is critical that families’ voices are centered in all reforms and that the NSW Government resource and fund Aboriginal community-controlled organisations to help Aboriginal people with high quality culturally safe and timely assistance before, during, and after all coronial processes.”
“With nine coronial matters currently on foot, it is critical that the NSW Government invest in a specialist ALS team to provide wraparound holistic support to families – who are forced to grieve and seek justice simultaneously.”
For more information and media enquiries:
Media contact: Sarah Puckeridge, caposecretariat@alc.org.au
As a young 47-year-old man, yet to hit the milestone of eldership, I reflect on two times in my life that feel worlds apart; my youth and now.
Always was Always will be were not words I heard as a young person, but as time goes on and my living status, memory and tradition changes, so have our conversations.
As a young man I grew up not fully understanding the true impact of who we are as people because our lives, through colonisation and policy, were controlled to a point whereby we were taught to think a certain way and put behind us the history of our ancestors.
I was never told our dream times stories but, as kids, we did practice a little of our traditional values and always had a high amount of respect for our elders. With the limited traditional values that were shared, we were never told the truth of who we really were as people to our own country.
The way I look at my childhood and the way I reflect upon it now, makes me feel frustrated that I was never told the truth. I can remember as a young person, that my life was good, I was happy, I had some really good friends, our family was accepted in community and I had really supportive parents, but years later I realised that the true story of our Aboriginal Australia was never told to us.
My memory through intergenerational history, tells me that what I wasn’t supposed to learn, was the truth of what I was meant to hear. History suppressed our memories.
I can remember sitting in my class in my Primary School days and singing songs such as, “toorali-oorali-addity, singing toorali-oorali-ay, singing toorali-oorali-addity, and we’re bound for Botany Bay.” I loved the tune. I sang this song with pride but never recognised until years later that I was actually singing a song that had no connection to me as an Aboriginal person. This was my childhood culture.
I experienced racism, had to fight for my independence, was oppressed to think another way, experienced intergenerational trauma through the removal of grandparents on my mother’s side and experienced the despair of dispossession.
I always knew I was Aboriginal and I always knew that my growing up was different, but it didn’t stop me from being who I am now. I now know more about my history, the pain, the suffering and the hurt that our ancestors went through and I allow this piece of history to motivate me to teach our kids and the wider community about our struggles and the true culture of being Aboriginal:
The dispossession,
The removal,
The racism,
The Policies,
The Government,
My people.
The culture you see today is not the culture of who we are. Traditionally, our values are represented through, spiritualty, kinship and connection to country. I cannot change history, but I can be involved in the truth-telling of our history. Always was, always will be.
Author – Phillip Naden, CEO of Coonamble and Dubbo AMS
On Thursday 29th of October 2020 AH&MRC visited Tharawal Aboriginal Medical Service (AMS). The visit was planned so that Sector Support and the Public Health and Intelligence Teams could share the projects they’ve been working on and brainstorm how AH&MRC can support Tharawal AMS with their programs and initiatives.
Tharawal AMS’s CEO, Darryl Wright took time out of his busy day to take the AH&MRC team on a tour of the service. He showed the AH&MRC Team the Fruit and Veg Shed where they run the ‘Good Tucker All Round Program’. This Fruit and Vegetable Delivery Program delivers boxes of fresh fruit and vegetables to Aboriginal and Torres Strait Islander people living on the Dharawal land in the Campbelltown Local Government Area. The program targets people who have or at risk of having a chronic disease including cardiovascular disease and diabetes.
Darryl introduced the Team to staff at Tharawal AMS and showed them around the Medical Centre, treatment rooms and Koori Garden, explaining all the healthy lifestyle programs that Tharawal AMS have to offer.
The team witnessed a special moment when Darryl presented a beautiful sculpture to a very hard-working staff member of the Poche Centre for Indigenous Health. The staff member had worked on the Poche bus all day making dentures for Tharawal AMS community members.
The AH&MRC team were impressed with the extensive services offered to Tharawal Community members in medical, social and emotional wellbeing, lifestyle and family support. It was a trip that we remember fondly in the years to come.
Author –
Marina Wise, AH&MRC Public Health and Intelligence Unit
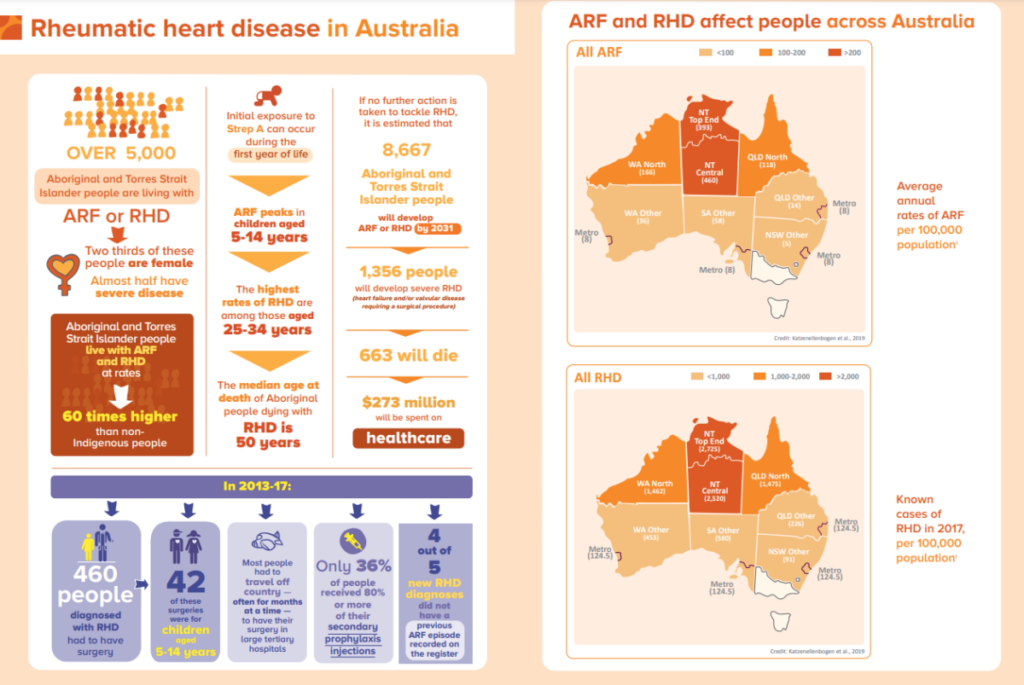
To many Australians, Rheumatic Heart Disease (RHD) is a foreign concept, a disease most will have never heard of. However, for Aboriginal and Torres Strait Islander people, RHD continues to pose a very real and present threat. Recent data from NSW public hospitals report the largest burden of disease occurs in children under the age of 15, followed by those between 15 – 29-year age group. Aboriginal people contributing to around 40% of cases in children aged less than 15 years.
Despite having been eliminated as a risk in the non-Indigenous Australian population for decades, RHD continues to devastate Aboriginal and Torres Strait Islander communities with some of the highest rates in the world. Learn more.
What is Acute Rheumatic Fever and RHD?
Acute Rheumatic Fever (ARF) is an illness that can occur after a throat or skin infection with the group A streptococcus bacteria. Episodes of ARF can cause permanent damage to heart valves, known as Rheumatic Heart Disease (RHD). Acute Rheumatic Fever and Rheumatic Heart Disease have been eliminated in most industrialized countries. However, in Australia ARF and RHD continue to affect specific high-risk groups, including Aboriginal and Torres Strait Islander people and people from countries where ARF is common.
Primary Prevention
It is very important that if you or your family have a sore throat or any concerns about skin health, that you ask your doctor to give you a check-up. Treating group A streptococcal infections quickly can prevent ARF and RHD from developing afterwards.
Group A streptococcal infections can be prevented by improving environmental conditions known to increase the risk of infection, such as good hygiene practices and improving living conditions including avoiding over-crowding.
Secondary Prevention
ARF can be treated with a series of antibiotic injections to prevent the heart from being affected and RHD from developing.
Injections are never fun but are important as they can prevent the serious consequences of RHD. If you or someone you know has had ARF, please ask them to see their doctor to see whether treatment is needed.
Tertiary Prevention
Sometimes it is hard to find a good cardiologist or other specialists to see, but your local AMS can help you research and find the right care for you. The best care for people with ARF and RHD requires a range of health services, such as oral health, maternal health, and cardiology. Read more about Rheumatic Fever and Rheumatic Heart disease.
Current training courses for healthcare professionals
Hospital grade hand sanitiser and reusable, cloth face masks will be distributed to Aboriginal Communities in NSW by the Aboriginal Health & Medical Research Council (AH&MRC) through their 47 Member Services.
“These protective measures remind Communities to remain vigilant as COVID-19 becomes the new normal, and testing rates drop in NSW. It is especially important as some people can be infectious with COVID-19 but show no symptoms,” said Robert Skeen, AH&MRC CEO.
“Cloth face masks offer a sustainable option for Aboriginal people to protect their families and Communities. They also reduce the financial burden of buying disposable masks. Spreading the messages about avoiding crowded places, washing hands regularly and wearing the masks is also important to keep Aboriginal Communities safe.”
The three-layered cloth face masks were purchased from an Indigenous supplier, Kulbardi. The masks meet NSW Health recommendations and include a water-resistant layer on the outside to give the best protection. The AH&MRC is pleased to see 1% of sales will go to the Bibbulman Fund – a Kulbardi initiative that designs and delivers programs around entrepreneurship, education numeracy and literacy to Indigenous Communities across Australia.
“From the start of this pandemic, AH&MRC has worked hard to make sure Aboriginal Medical Services can access enough supplies of personal protective equipment (PPE) such as gowns and masks to continue their response,” said Robert Skeen. “We appreciate the support of NSW Health in helping us provide supplies to our Member Services. We will continue to advocate for more sector funding to guarantee the best health outcomes for Aboriginal people.”
Along with keeping 1.5 metres apart, getting a COVID-19 test, wearing a mask is one of several precautionary measures Aboriginal Communities can take to prevent the spread of COVID-19. With COVID-19 testing rates low in NSW, AH&MRC strongly encourages anyone with flu-like symptoms to immediately have a COVID-19 test. Find the nearest NSW COVID-19 testing clinic here.
For more information visit the NSW Health website or download AH&MRC’s brochure: Frequently Asked Questions on Cloth Face Masks.
Aboriginal Health & Medical Research Council is not for profit organisation working to support Aboriginal Community Controlled Health Services to deliver better health outcomes for Aboriginal people in NSW.
Thanks to the fast work of the Tharawal Aboriginal Corporation (TAC) team, the Aboriginal community of Campbelltown in south-western Sydney, have remained COVID-safe. More than 11,200 Aboriginal people live in South Western Sydney Local Health District (SWSLHD) and 3,405 Aboriginal people attend Tharawal for their primary health care. Caring for the Aboriginal community is what the TAC team do, but at no time has this care been more important, than during the COVID-19 pandemic. Following the outbreak of COVID-19 in south western Sydney, the team established a drive-through and walk-in testing service for the Aboriginal and wider community at Airds, for a four-week period. These actions were in response to an increase in COVID-19 cases in the area and the need for broader testing to detect additional cases. The team managed to pull together all elements required and the clinic was fully operational within two working days. The agility and timeliness of the response is an example of the strong partnership Tharawal has with SWSLHD.
Additional staff from SWSLHD provided their support at the clinic. With support from Histopath, the clinic has now tested more than 1500 people. Tharawal’s Chief Executive, Darryl Wright and his team, worked tirelessly adapting to meet the community’s needs in what was already a very challenging time for health service delivery.
‘This is a deadly virus, but we are more deadly,’ Mr Wright said.
Tharawal GP Dr Bemand said this is no time to relax. ‘The community needs to maintain vigilance in practising COVID-safe behavior,’ said Dr Bemand. Recognising the ongoing threat of COVID-19, Tharawal will continue to offer testing to the community through their regular GP Clinic to ensure the community remains COVID-safe.
After months working as socially distanced desk-jockeys, the AH&MRC’s Public Health Team hit the road once more to visit Members Services including Illawarra Aboriginal Medical Service (IAMS), South Coast Medical Services Aboriginal Corporation (SCMSAC) and Waminda – South Coast Women’s Health & Welfare Aboriginal Corporation. The crew included Kezia Blackledge, Marina Wise, Victoria Kennedy, and Nina Betts. They were joined by Nathan Taylor from Program of Experience in the Palliative Approach (PEPA). The team wanted to check in and see how Services had been travelling over the last few months, and have a yarn about their Nicotine Replacement Therapy (NRT) programs, palliative care, sexual health and Your Health, Your Future initiatives.
NRT helps clients quit their own way
Despite the challenges of the pandemic, the Services are using creative ways to stay on top of their NRT distribution.
At the South Coast AMS, the Tackling Indigenous Smoking (TIS) team have started a numbered voucher system, with participating chemists in Nowra, Jerringa and Wreck Bay. Once clients are screened by the TIS team, they can visit their local chemist and present the voucher – with different vouchers for different types of NRT. If vouchers are missing the team will follow up with their clients. This helps the TIS team identify any barriers that could prevent clients going to their local pharmacy, and resolve any issues they may be facing, such as lack of transport.
At Waminda, having NRT stock on hand allows staff to provide immediate treatment. Once a client has been screened, providing NRT on the spot helps keep Community members engaged and motivated to quit smoking. Other strategies at Waminda include delivering the NRT, staff capacity building and actively following up with clients to see how they are going.
At IAMS, NRT is well embedded into clients’ quit journeys, which has enabled them to keep service provisions strong despite the COVID-19 pandemic. The IAMS team also surprised us with some deadly face masks designed by a local artist.
Understanding what is needed for palliative care support
The trip provided an opportunity to share AH&MRC’s latest palliative care project ‘Journey to Dreaming.’ This project aims to develop two resources; a Toolkit and Diary for Member Services, their clients, and families to find culturally appropriate support in these sensitive and sad times.
Our Member Services want to support their community as much as they can and shared their ideas to develop culturally appropriate and meaningful Journey to Dreaming resources. Some of these ideas included; offering smoking rooms, large gatherings of mob during and outside usual visiting hours, wills, funerals, Advance Care planning, family support, a space to write down important phone numbers, appointment times, an activity section, your feelings for the day, messages to your family, the types of treatment you might be receiving, and a reflection page. We look forward to working with our Members to develop the right resources and programs for the Journey to Dreaming project.
Working together on sexual health
AH&MRC staff, Keiza and Marina, had a yarn with Member Services about AH&MRC’s upcoming sexual health project. Members had the opportunity to suggest key topics they would like to include as part of the new program. The team at IAMS shared how this project can blend sexual health information with a strong cultural perspective. Waminda was interested to collaborate and develop sexual health resources for the benefit of all Member Services. The Public Health Team valued the opportunity to listen and work alongside our Members Services.
“We left the meeting in high spirits knowing we are addressing our Members’ needs and can work together from the beginning of a new project. This is the best way to truly collaborate and deliver meaningful, culturally appropriate sexual health resources for their Communities.” – AH&MRC’s Public Health Team
Strengthening the Your Health, Your Future campaign
The team delivered Your Health, Your Future merchandise including tote bags, skipping ropes, frisbees and balls to Member Services for their Communities. Kids can have fun while staying active. It helps raise awareness for the Your Health Your Future campaign that encourages people to make the right decisions about their health, for their future. Members shared feedback on 715 Aboriginal and Torres Strait Islander Health Assessments during COVID-19. Despite the outbreak, Members have encouraged Community members to visit their Services for a health assessment as the first step to looking after their health today, and tomorrow.
“We were able to get Members’ deadly feedback on ways to improve the Your Health, Your Future program. We will work to get a stronger message out to Community on the benefits of having a health assessment at their local AMS.” – AH&MRC’s Public Health Team
About the author: Reuben Morrison-Greet is a 21 year old paramedic student who is passionate about Indigenous health. Rueben raised $1,330 for the AH&MRC by setting up a fundraiser for his cycling trip from Sydney to Broken Hill. No small feat, the cycling trip is over 1000 km away and took 8 days. The AH&MRC and our Member Services are grateful to Reuben and his contribution to Aboriginal health in NSW.
Day 1.
I remember standing in my kitchen, staring outside at the dark, pouring rain. “It’s an awfully long way,” my mum said, standing next to me. It was 6 am on a Sunday morning and, that day, I was going to embark on an 1000km cycling trip from Sydney to Broken Hill. I was on a tight schedule as I planned to catch a train back from Broken Hill to Sydney in 8 days time.
But first I had to get there.
My Trip from Sydney to Broken Hill
After resisting the urge to crawl back into bed, I rolled my bike out of the garden and started off towards the city. I pedalled through the morning traffic, over the ANZAC bridge, then Parramatta road. With a sleeping bag, mat, stove and everything else I needed for my weeklong journey strapped to my bike, I set my course for Lithgow.
A fully loaded bicycle, a home away from home!
My growing curiosity on the topic of Indigenous health developed when I initially started my degree in health science, where I would find myself continually getting side-tracked during assignments. After reading articles about how Australia has one of the highest performing healthcare systems in the world, my eyes were often drawn to the little asterisk that always footnoted the too often undiscussed reality; “*For non-indigenous Australians”. It was only after I started down the trail of scientific articles, government reports, historical recounts, or coroners’ findings, that I would begin to grasp the scale and historical depth of these continued injustices that are still reflected today.
After some hair raising moments riding up and over the Blue Mountains, I crawled into a cheap pub room, ate a greasy dinner, and ended up shorting-out the entire upper floor of the pub in an attempt to dry my soaking wet gear with an electric heater.
Day 2.
The weather was marginally better; consistent rain accompanied by narrow highway shoulders and heavy trucks made for a stressful ride to Orange. A puncture in my tyre and a friendly chat with a bike shop owner helped break the monotony.
Day 3.
I decided to take a break from the bike to manage an ongoing injury and instead caught a bus to Condobolin. I struck up a conversation with a man in a pub and mentioned where I planned on stopping the following day; Murrin Bridge, an Indigenous community. I could write a whole separate blog on this conversation alone, but I’ll just say that it left a very bitter impression after realising that particular discriminatory attitudes towards Indigenous Australians were very much alive.
I set out after dinner and rode into the night, setting up my sleeping gear and sleeping bag cover by the side of the road.
Day 4.
As highways turned into single-lane roads, I suffered another punctured tyre coming into Euabalong. After asking around the town for some sealant, within 5 minutes I found myself explaining the unique design differences between Presta and Schrader bicycle tube valves to the entire council road works team at their Euabalong depot.
Hillston to Ivanhoe. Can you spot the car?
Euabablong West.
After kindly declining a “short trip” up to Cobar, I continued to Murrin Bridge. I called ahead in the days prior to make sure the community centre knew I was stopping by, but it was still a surprise to be ushered inside and served a hot lunch within seconds of arriving. I was then introduced to a resident who gave me brief history and tour of what it was like growing up in Murrin Bridge.
Murrin Bridge Community. Ex-Mission
What’s more impressive? A bucket full of emu eggs or 4 days’ worth of helmet hair?
Myself and a proud Murrin Bridge Resident, born and bred.
Murrin Bridge Community Centre
The brief mention of “dogs might chase you” after my walk around was enough to have me promptly on my way to Lake Cargelligo. After a brief stop at the scenic Lake Cargelligo, a glowing red sunset turned into night riding as I pulled into Hillston at about 8pm.
Day 5.
Hillston to Ivanhoe. Empty but difficult dirt roads. 360-degree horizon views. Turns out a name on a map isn’t always a town (looking at you, Mossgiel). If anyone finds a pair of black rain pants on this stretch of road, let me know.
Hillston to Ivanhoe. Can you spot the car?
Nothingness. You can see a car approaching from about 5 mins away.
Day 6.
I had a planned a half- rest day at Ivanhoe due to bad weather, turns out; there was a rugby match on that had attracted about 1000 people that night. Safe to say, as a mixed-race city kid wearing Lycra on a bicycle, I stuck out like the sorest of sore thumbs. Minus the matching Hi-Vis.
1/2 of food options available in Ivanhoe. This place was crammed with patrons the previous night.
Enough food and 3L of water to last 200km
Day 7.
Ivanhoe to Menindee. 160km dirt road. Isolated and vast, but clear skies. Sand and clay definitely test your patience.
My sleeping setup. About 40kms out of Ivanhoe
Day 8.
Menindee to Broken Hill. Homestretch! Ran out of water with 40kms to go. Oops. Low tyre pressures from the day before + misplaced handpump = picking your bike up and walking it over cattle grids – how embarrassing.
70kms! Not long now..
Broken Hill! I should have taken this somewhere more iconic, lucky the Harvey Norman Truck has Broken Hill written on it…
The early train back to Sydney. But first some deodorant…