
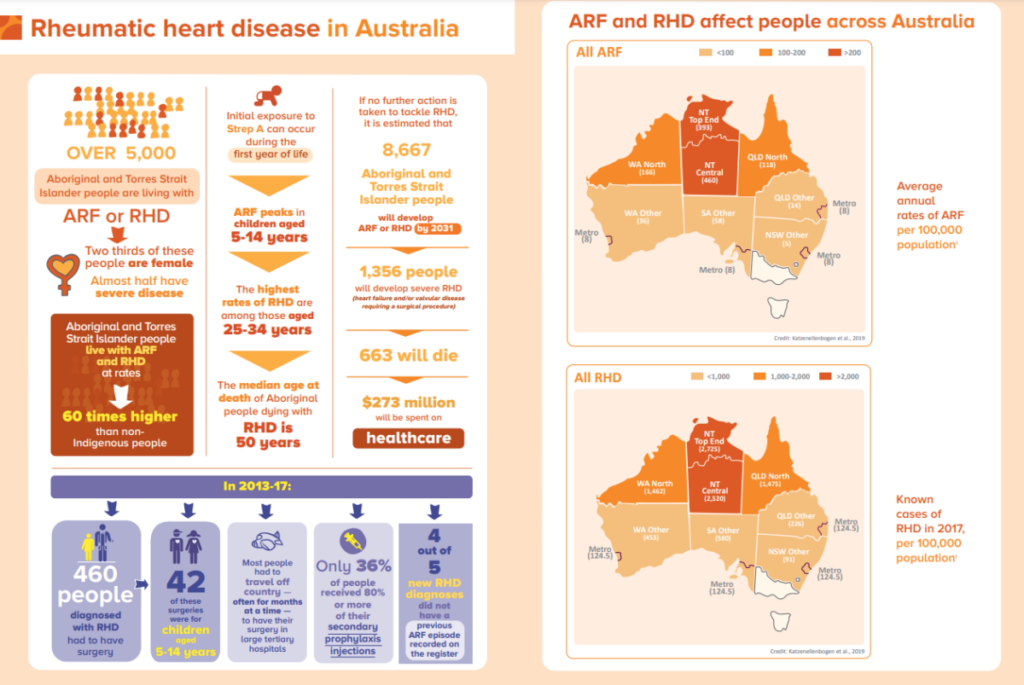
To many Australians, Rheumatic Heart Disease (RHD) is a foreign concept, a disease most will have never heard of. However, for Aboriginal and Torres Strait Islander people, RHD continues to pose a very real and present threat. Recent data from NSW public hospitals report the largest burden of disease occurs in children under the age of 15, followed by those between 15 – 29-year age group. Aboriginal people contributing to around 40% of cases in children aged less than 15 years.
Despite having been eliminated as a risk in the non-Indigenous Australian population for decades, RHD continues to devastate Aboriginal and Torres Strait Islander communities with some of the highest rates in the world. Learn more.
What is Acute Rheumatic Fever and RHD?
Acute Rheumatic Fever (ARF) is an illness that can occur after a throat or skin infection with the group A streptococcus bacteria. Episodes of ARF can cause permanent damage to heart valves, known as Rheumatic Heart Disease (RHD). Acute Rheumatic Fever and Rheumatic Heart Disease have been eliminated in most industrialized countries. However, in Australia ARF and RHD continue to affect specific high-risk groups, including Aboriginal and Torres Strait Islander people and people from countries where ARF is common.
Primary Prevention
It is very important that if you or your family have a sore throat or any concerns about skin health, that you ask your doctor to give you a check-up. Treating group A streptococcal infections quickly can prevent ARF and RHD from developing afterwards.
Group A streptococcal infections can be prevented by improving environmental conditions known to increase the risk of infection, such as good hygiene practices and improving living conditions including avoiding over-crowding.
Secondary Prevention
ARF can be treated with a series of antibiotic injections to prevent the heart from being affected and RHD from developing.
Injections are never fun but are important as they can prevent the serious consequences of RHD. If you or someone you know has had ARF, please ask them to see their doctor to see whether treatment is needed.
Tertiary Prevention
Sometimes it is hard to find a good cardiologist or other specialists to see, but your local AMS can help you research and find the right care for you. The best care for people with ARF and RHD requires a range of health services, such as oral health, maternal health, and cardiology. Read more about Rheumatic Fever and Rheumatic Heart disease.
Current training courses for healthcare professionals
RHD Australia are conducting new and free e-learning courses designed for clinicians who care for Aboriginal and Torres Strait Islander people living with RHD. Learn more about RHD Australia’s Training courses here.
Educational courses on prevention, diagnosis and management of ARF and RHD include:
- Introduction to Acute Rheumatic Fever and Rheumatic Heart Disease
- RHD for community-based workers
- Women and girls with RHD
Author
– Marina Wise, Public Health Officer